
By Denise Grady
Delicate procedure offers a chance at pregnancy for thousands of women
Six doctors swarmed around the body of a newly deceased organ donor and quickly started to operate.
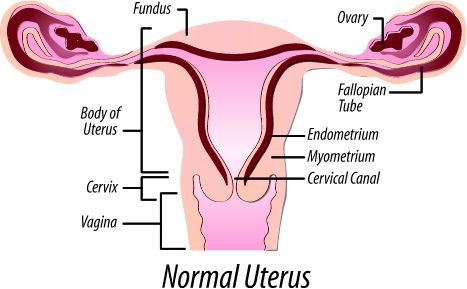
The kidneys came out first. Then the team began another delicate dissection, to remove an organ that is rarely, if ever, taken from a donor. Ninety minutes later they had it, resting in the palm of a surgeon’s hand: the uterus.
The operation was a practice run. Within the next few months, surgeons at the Cleveland Clinic expect to become the first in the United States to transplant a uterus into a woman who lacks one, so that she can become pregnant and give birth. The recipients will be women who were born without a uterus, had to have it removed or had uterine damage. The transplants will be temporary: Each uterus will be removed after the recipient has had one or two babies, so she can stop taking transplant-rejection drugs.
Uterine transplants are a new frontier, one that brings together specialists in two fields known for innovation and for pushing limits, medically and ethically: reproductive medicine and transplant surgery. If the procedure works, many women could benefit: An estimated 50,000 women in the United States lack a uterus. But there are potential dangers.
The recipients, healthy women, will face the risks of surgery and anti-rejection drugs for a transplant that they, unlike someone with heart or liver failure, do not need to save their lives. Their pregnancies will be considered high risk, with their fetuses exposed to antirejection drugs, and developing inside a womb taken from a dead woman.
Eight women from around the country have begun the Cleveland Clinic’s screening process, hoping to be selected for transplants. One, a 26-year-old mother of two adopted children, said she still longed for a chance to become pregnant and give birth.
‘‘I crave that experience,’’ she said. ‘‘I want the morning sickness, the backaches, the feet swelling. I want to feel the baby move. That is something I’ve wanted for as long as I can remember.’’
She had traveled more than 1,000 miles to the clinic, paying her own way. She asked that her name and hometown be withheld to protect her family’s privacy.
She was 16 when medical tests, performed because she had not begun menstruating, found that she had ovaries but no uterus — a syndrome that affects 1 in 4,500 newborn girls. She came from a large family, and had always assumed she would have children. The test results were devastating.
‘‘There are women who won’t adopt or have surrogates, for reasons that are personal, cultural or religious,’’ said Dr. Andreas G. Tzakis, the driving force behind the project and the director of solid organ transplant surgery at the Cleveland Clinic’s hospital in Weston, Fla. ‘‘These women know exactly what this is about. They’re informed of the risks and benefits. They have a lot of time to think about it, and think about it again. Our job is to make it as safe and successful as possible.’’
The hospital plans to perform the procedure 10 times, as an experiment, and then decide whether to continue. Dr. Tzakis said he hoped to make the operation readily available in the United States.
Sweden is the only place in the world where uterine transplants have been done successfully. Nine women have had them — all with a uterus from a live donor — at the University of Gothenburg, and four have given birth, the first in September 2014. Another is due in January. Their babies were born healthy, though prematurely. Two transplants failed and had to be removed, one because of a blood clot and the other because of infection.
Earlier attempts — one in Saudi Arabia, one in Turkey — failed. Other hospitals in the United States and Britain are now also preparing to try the surgery, but are not as close as the team in Cleveland.
Dr. Tzakis said thousands of women with kidney or liver transplants, who must continue taking anti-rejection drugs during pregnancy, had given birth to healthy babies, indicating that the drugs are safe. Those women are more likely than others to have preeclampsia, a complication involving high blood pressure, and their babies tend to be smaller. But it is not known whether those problems are caused by the drugs, or by the underlying illnesses that led to the transplants. Dr. Tzakis said that because women receiving uterine transplants would be healthy, he was hopeful that complication rates would be very low.
A medical ethicist not connected with the research, Jeffrey Kahn, of Johns Hopkins University, said the procedure did not set off any alarms with him.
‘‘We’re doing lots of things to help people have babies in ways that were never done before,’’ Dr. Kahn said. ‘‘It falls into that spectrum.’’
Dr. Tzakis, 65, said he had performed 4,000 to 5,000 transplants of kidneys, livers and other abdominal organs. To prepare for the uterine surgery, he spent time with the Swedish team, practicing in miniature swine and baboons and observing all nine of the human transplants in the operating room.
He described transplantation as ethically superior to surrogacy, saying that with surrogacy ‘‘you create a class of people who rent their uterus, rent their body, for reproduction. It has some gravity. It possibly exploits poor women.’’
The Swedish team used live donors, and showed that a uterus from a woman past menopause, transplanted into young recipient, could still carry a pregnancy. In five cases the donor was the recipient’s mother, which raised the dizzying possibility of a woman giving birth from the same womb that had produced her.
The Cleveland doctors will use deceased donors, to avoid putting healthy women at risk. For a live donor, the operation is far more complicated than a standard hysterectomy and takes much longer, seven to 11 hours, Dr. Tzakis said, adding, ‘‘You have to work near vital organs.’’
The surgeons have to remove part of the donor’s vagina and other tissue they will need to attach the uterus to the recipient. And they must tease away tiny blood vessels without harming the donor. The uterine vessels are wound around the ureters, which carry urine from the kidneys to the bladder. ‘‘They’re like worms wrapped around a tube,’’ Dr. Tzakis said. ‘‘It’s very tedious to separate them.’’
With deceased donors, there is no need to worry about injuries. The organ can be removed faster, and can survive outside the body for at least six to eight hours if kept cold.
For a recipient of the uterus, the process will be long and complicated. To be eligible, candidates must be in a stable relationship, because they will need support. They must also have ovaries.
The initial phase includes screening for psychological disorders or marital problems that could interfere with their ability to cope with a transplant and be part of a study. Candidates are also questioned to make sure that no one is pressuring them to have the transplant. Doctors use similar criteria for people receiving other types of organ transplants because the process is arduous, and patients with a strong social support system seem to fare better.
Finances matter, too, because during parts of the study, recipients will have to live in Cleveland, and those from out of town will have to pay for their own food and lodging.
Because the fallopian tubes will not be connected to the transplanted uterus, the recipients will go through in-vitro fertilization.
Before having the transplant, the woman will take hormones to stimulate her ovaries to produce multiple eggs. Ten will be needed, so she may have to go through more than one cycle of hormone treatment. Doctors will collect the eggs, fertilize them with her partner’s sperm and freeze them. Once there are 10 embryos in the freezer, the woman will be put on the waiting list for a transplant from a deceased organ donor.
When a donor with matching blood and tissue type becomes available, the transplant will take place.
The woman will wait one year to heal from the surgery and adjust the doses of anti-rejection medicine before trying to become pregnant. Then doctors will perform in-vitro fertilization, implanting one egg at a time in the uterus, until the recipient becomes pregnant. The baby will be delivered by cesarean section before the due date, to protect the transplanted uterus from the strain of labor.
After giving birth, the mother can either keep the uterus to have one more baby (two is the limit, for safety reasons), or have it removed so she does not have to take the anti-rejection drugs anymore. If she does not want to have the surgery, doctors said, it may be possible just to quit the drugs and let the immune system reject the uterus, which should then gradually wither away.
One of the surgeons working with Dr. Tzakis will be Dr. Tommaso Falcone, the clinic’s chairman of obstetrics and gynecology. Dr. Falcone said he first heard of uterus transplants about 10 years ago, when early research was described at medical conferences. Initially, he was skeptical.
A trip to Sweden changed his mind. He flew there in 2013 — like a doubting Thomas, he said — to see for himself what the team was doing. He watched the surgery, and spoke to several couples who wanted it.
‘‘I almost cross-examined them,’’ Dr. Falcone said. ‘‘I was thinking, ‘There’s got to be something wrong with these people.’ ’’
But, he said, he came to understand how much pregnancy meant to them.
‘‘It’s a legitimate request,’’ he said. ‘‘I got on the plane and knew I would be at the forefront of trying to make this program work at the Cleveland Clinic.’’
Source: International New York Times
Get more stuff like this
Subscribe to our mailing list and get interesting stuff and updates to your email inbox.


















{kind=link}